

Let’s delve into the world of Tuberculosis with insights from Dr. Parthiv Shah, a renowned TB specialist in Mumbai. Tuberculosis (TB) is caused by Mycobacterium tuberculosis, a bacterium that can affect any part of the body. Understanding the distinction between latent TB infection (LTBI) and TB disease is crucial, as untreated TB disease can be fatal.
Latent Tuberculosis Infection (LTBI)
Latent Tuberculosis Infection (LTBI) is characterized by the presence of TB bacteria in the body, albeit in an inactive state. Individuals with LTBI typically do not exhibit any symptoms and are unable to transmit TB to others. Diagnosis of LTBI is usually confirmed through a positive TB skin or blood test.
TB Disease
- Definition: Active growth of TB bacteria, often in the lungs.
- Symptoms: Cough, chest pain, weight loss, fever, night sweats.
- Transmission: Contagious, requiring prompt treatment.
Diagnostic Tests for TB
Dr. Parthiv Shah offers a range of diagnostic tests for TB, including TB skin tests, smear tests, culture tests, and drug sensitivity testing.
TB Skin Test
- Purpose: To detect TB infection.
- Procedure: Injection of tuberculin under the skin.
- Interpretation: Positive reaction indicates TB infection.
Smear and Culture Tests
- Smear Test: Detects TB bacteria in sputum within a day.
- Culture Test: Identifies TB bacteria in sputum or body fluids in 4-6 weeks.
Drug Sensitivity Testing
- Importance: Determines effective drugs for TB treatment.
- Crucial for: Managing drug-resistant TB cases.
Treatment for TB Disease
The treatment approach for TB disease varies based on severity and drug sensitivity.
Drug-Sensitive TB (DSTB)
- Regimen: 2HRZE/4HRE for H & R sensitive TB cases.
- Phases: Intensive phase (IP) and continuation phase (CP).
- Duration: Tailored based on TB type and patient response.
Drug-Resistant TB (DR TB)
- Regimens: All-oral H mono/poly DR TB regimen, shorter MDR TB regimen.
- Expertise: Dr. Parthiv Shah specializes in managing complex TB cases.
| Type of TB Case | Treatment Regimen in IP | Treatment Regiment in Cp |
| New & Previously treated case (H & R sensitive/ unknown) | 2 HRZE | 4 HRE |
Regimen for DR TB treatment :
Under NTEP, the following are the standard DR TB regimens:
1. All oral H mono/poly DR TB regimen
2. Shorter MDR TB regimen
3. All oral longer MDR TB regimen
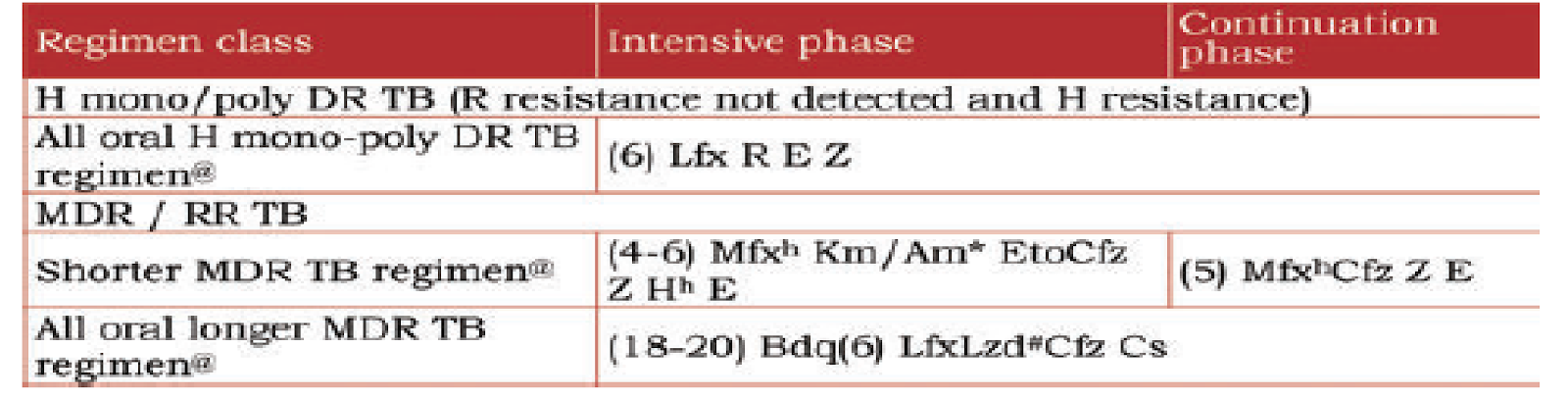
Lfx – levofloxacin, Mfx – moxifloxacin, Km – Kanamycin, Am – Amikacin , Eto – ethionamide, Cfz – Clofazimine, Bdq – Bedaquilline, Lzd – Linezolid, Cs – Cycloserine
Prevention of TB
Preventive measures play a vital role in controlling the spread of TB.
BCG Vaccine
- Purpose: Given to infants in high TB burden areas.
- Effectiveness: Reduces severe forms of TB in children.
Contact Tracing
- Importance: Identifying and treating individuals in close contact with TB patients.
- Role: Essential for preventing community spread of TB.
Understanding Tuberculosis, its diagnostic methods, treatment options, and preventive strategies is crucial in combating this infectious disease. Consult a TB specialist like Dr. Parthiv Shah for comprehensive care and management of TB cases. Stay informed, stay healthy!
Dr. Parthiv Shah, the best pulmonologist in Mumbai, is here to help you to know more about Tuberculosis. Book your appointment today at Sparsh Superspeciality Lung Clinic and take the first step towards better lung health by calling +91 90297 72904.